Em 1896, Henri Becquerel descobriu uma nova radiação enigmática. Ao contrário dos raios X que desapareciam quando o tubo dos mesmos era desligado, esta radiação observada do Urânio era emitida continuamente. Estudos mais aprofundados levados a cabo por Pierre e Marie Curie relevaram que existiam outros elementos que possuíam a mesma propriedade. Em particular, descobriram estas propriedades no polónio e no rádio, em 1898.
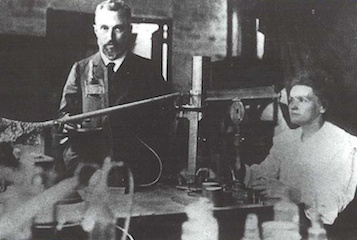
Pierre e Marie Curie rapidamente encontraram uma utilização para esta propriedade e, já em 1901, o rádio estava a ser utilizado em hospitais. Sabia-se que a radiação proveniente do rádio possui efeitos benéficos para muitas doenças cutâneas, inclusivamente o cancro.
Pierre e Marie Curie no seu laboratório, Paris 1898.
A nova radiação era de origem nuclear. Alguns núcleos emitem espontaneamente partículas α (núcleos de hélio), partículas β – estas podem ser eletrões (β-) ou positrões (β+) – e/ou radiação γ (gama) (i.e., fotões de alta energia). Um átomo com um núcleo instável, caracterizado por possuir uma energia excessiva é designado como radionuclídeo, nuclídeo radioativo, ou ainda radioisótopo ou isótopo radioativo.
Exemplos de radioisótopos naturais são o 238U (urânio), 40K (potássio), 232Th (tório) e os seus núcleos-filho 226Ra (rádio), 222Rn (rádon), 218Po (polónio). Alguns radioisótopos são continuamente produzidos por ação da radiação cósmica nas camadas mais superiores da nossa atmosfera, como por exemplo, 14C (carbono), 3H (trítio) ou 7Be (berílio).
Irene e Frederic Joliot-Curie foram os primeiros a produzir radioisótopos artificiais em 1933, ao utilizarem uma fonte- α natural para bombardear alumínio-27 e produzir o elemento radioativo fósforo-30 que decai por radiação-β para silicone-30. Este foi o resultado dos núcleos dos átomos de alumínio ao receberem protões adicionais a partir de núcleos de hélio (partículas α).
Desde então, muitos novos radioisótopos têm sido produzidos, alargando o número de novas aplicações e conduzindo a uma melhor compreensão da matéria nuclear e das forças nucleares. Por volta de 1936, já 200 radionuclídeos tinham sido produzidos. Atualmente são conhecidos cerca de 2500. São produzidos utilizando feixes de partículas, que vão desde protões ao 238U, acelerados em ciclotrões ou em aceleradores lineares.
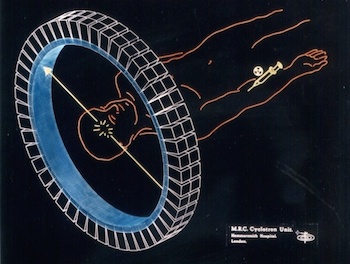
O primeiro acelerador (ciclotrão) foi construído em Berkeley, nos Estados Unidos em 1932 por Ernest O. Lawrence. Ele e o seu irmão John Lawrence - médico - rapidamente reconheceram aplicações médicas de grande importância, e produziram isótopos radioativos para investigações biológicas e médicas, bem como para o tratamento de cancros. O primeiro ciclotrão Europeu foi construído por Frederic Joliot (1939) no College de France, Paris.
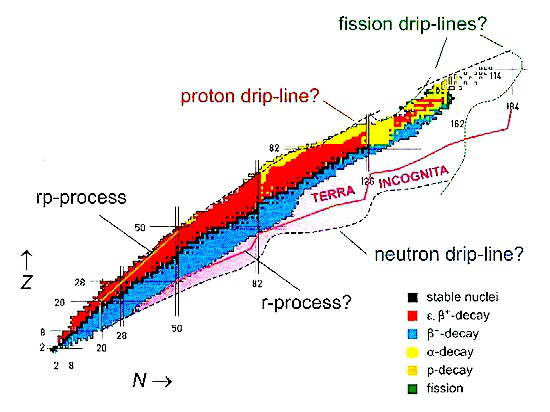
Físicos têm produzido muitos novos isótopos que se encontram cada vez mais afastados do vale da estabilidade nuclear natural. Atualmente, existem muitas instalações que utilizam feixes de iões radioativos. A procura de radioisótopos para fins medicinais é um fenómeno mundial, e nos países desenvolvidos tem vindo a crescer exponencialmente desde 1995.
O prémio Nobel da Química de 1943 foi atribuído a G. de Hevesy por ter sido o pioneiro no uso de elementos radioativos naturais (e mais tarde artificiais) como traçadores no estudo de elementos estáveis em sistemas biológicos. Uma pequena quantidade de um elemento radioativo pode ser facilmente observada no corpo humano. Isto também é conseguido através de traçadores químicos, porém seria necessária uma maior quantidade de químicos, o que levaria ao aumento de risco do procedimento para o paciente.
Tipicamente, numa investigação medicino-nuclear um traçador é administrado ao paciente e os raios γ emitidos pelo traçador nuclídeo são registados com uma matriz de detetores de radiação. Este processo é chamado de tomografia por emissão. O marcador é frequentemente escolhido de modo a que este se deposite seletivamente num órgão particular, e que depois os raios γ detetados forneçam uma imagem detalhada da região de interesse. Para um olhar experiente, as imagens podem revelar anomalias estruturais ou metabólicas conduzindo a melhores diagnósticos. Na medicina nuclear há uma grande quantidade de isótopos que são utilizados, cada um destinado especificamente para os órgãos individuais do corpo humano.
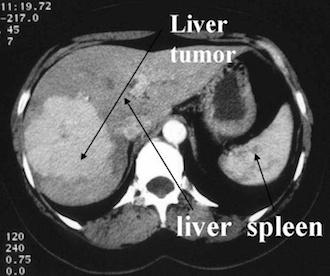
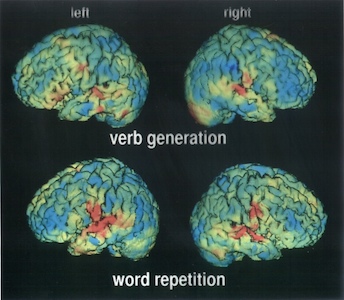
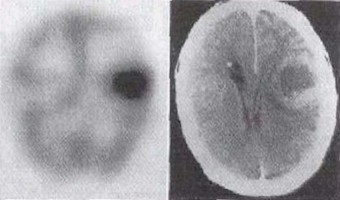
Imagem acima: aplicação de PET em neurofisiologia (exercício de memória verbal no cérebro), Hospital San Raffaele, Milão.
Os tumores podem ser diagnosticados através de técnicas como a Tomografia Computorizada por Emissão de Fotão Único (SPECT) ou a Tomografia por Emissão de Positrões (PET) (em que núcleos emissores de positrões (β+) são utilizados para produzir – por um processo de aniquilação – raios γ energéticos). As técnicas de SPECT e PET são típicas em diagnóstico de tumores, bem como em estudos funcionais do cérebro normal saudável.
Imagem de uma tomografia computorizada usando raios-X a partir de um marcador de iodeto (Hospital Erasme, Bruxelas).
Entre os elementos radioativos, o Iodo (I) tem um papel único, já que este se liga ao tecido da tiroide com grande afinidade e seletividade. Para doses reduzidas pode ser utilizado para fins diagnósticos, ou, alternativamente, podemos proceder ao tratamento do cancro da tiróide aproveitando a radiação emitida do Iodo radioativo, que se ligada exclusivamente a tecidos da tiróide.
131I (radiação β e γ, com um tempo de meia-vida de 8 dias) tem sido utilizado há mais de 50 anos para o estudo da atividade da tiróide. Tc-99m (um estado metaestável excitado do núcleo de tecnécio-99 com um tempo de meia-vida de 6 horas) é também um bom marcador usado para o estudo de órgãos como o cérebro, o fígado e os pulmões. O rádio e o estrôncio são usados no estudo dos ossos e do esqueleto.
Os elementos químicos fisiologicamente mais intrigantes como o C (carbono), N (nitrogénio) e o O (oxigénio) apresentam emissões β+ de isótopos de curta vida usados em técnicas de PET. Os nuclídeos de emissão beta normalmente utilizados são 11C, 13N, 15O e 18F (flúor).
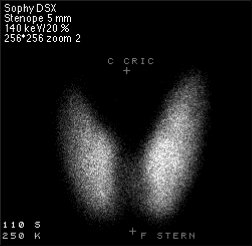
Imagem à direita: Cintigrafia da atividade da tiroide usando tecnécio.
SPECT stands for Single Photon Emission Computed Tomography. In this procedure, organs are imaged by measuring the distribution of an injected radio-tracer by means of a gamma 'camera' linked to a computer. SPECT imaging involves the rotation of a gamma detector array around the patient to acquire measurements from multiple angles. With this technique, the position and the concentration of radionuclide distribution is sought. SPECT involves the use of radioisotopes like 99mTc, or 123I where a single γ (of 140 keV) is emitted.
There are many applications of SPECT both in and as a therapy aid. SPECT scans using a radioisotope not absorbed by tissues but instead travelling in the bloodstream can be used to see how blood flows to certain tissues and organs. This is particularly useful for scans of the brain and heart.
In the Positron Emission Tomography (PET) technique, commonly used isotopes are 15O, 13N, 11C and 18F. These have short half-lives of about 2, 10, 20.4 and 110 min, respectively, so the radioisotopes have to be produced close to where they’re used. For this reason, many hospitals have a small cyclotron nearby or even within the hospital itself, specially constructed to produce these isotopes. The isotope is then attached to a natural chemical such as glucose, water or ammonia which is then put into the human body via an injection or possibly by breathing it in as a gas. The radioisotope travels to the part of the body that uses the chemical it was attached to, which is why many different types of chemicals are used.
Elementary particles have corresponding anti-particles. A particle’s anti-particle is effectively the same particle but with the opposite electrical charge. When a particle and its anti-particle collide, they annihilate with the emission of pure energy.
The isotopes typically used in a PET scan are β+ emitters. When the isotope decays inside the patient's body, any emitted positron (β+) travels only a short distance in the tissue (typically less than 1 mm, but this dependeds on the isotope) before it annihilates with an electron (β-). The energy released at the annihilation is in the form a pair of gamma (γ) photons emitted at 180° with respect to each other, and an energy of 511 keV each. The detection of the two γ rays in coincidence by two detectors allows one to localise the decay event on the line connecting the two detectors.
PET scans are commonly used to diagnose cancers, heart conditions and some brain disorders like epilepsy or Alzheimer’s disease. PET is also employed in assessing the response to cancer therapy. In addition, PET scans are used in research, for example studies of the effects of drug abuse or ageing.
The risks associated with a PET scan are very small but as with most types of scans, it’s not always suitable for pregnant or nursing women. Due to the presence of a radioactive substance in their body, hospitals advise patients to not to have any close contact with pregnant women or young children for at least a few hours after a PET scan.
PET scan image showing bone cancer of the skeleton (Hospital Erasme, Bruxelles).SPECT imaging is inferior to PET in terms of attainable resolution and sensitivity. For PET the best spatial resolution cattaineble presently is of about 6 mm, that is 2 to 3 times better than with SPECT. Because of their rapid decay, essentially all PET isotopes must be produced on the premises (with the exception of 18F of 110 min half-life). In contrast, SPECT isotopes like 123I have a sufficiently long half-life (13.2 hrs) to allow centralised production at distant sites with delivery then via express mail.
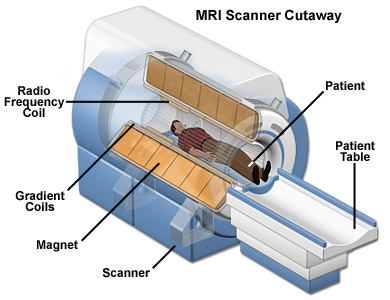
The main benefit of MRI is that it’s doesn’t use any radioactive substance. MRIs show the distribution of water (H2O) in the body and the organs where it is stored. The MRI is basically a large tube with powerful magnets inside. When a magnetic field is applied around the patient (which is not harmful) all the protons (hydrogen nuclei) in the water are pulled in one direction. When the proton snaps back into position it releases radio waves which the MRI scanner can then detect and measure to make a 2D image of the body. MRIs are commonly used for brain or heart diagnoses but can be used to scan almost any part of the body.
MRI technology is further being developed to address a wider range of clinical diagnosis problems. For example, polarised Xe-129 or He-3 can be used to image the airways in the lungs with high spatial and temporal resolution.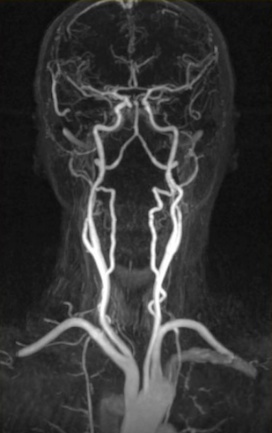

The 2003 Nobel Prize for medicine was awarded to to Paul Lauterbur and Sir Peter Mansfield for their work and contribution to Magnetic Resonance Imaging.
Most modern and academic hospitals nowadays employ MRI and PET, along with other imaging techniques. In many Nuclear Physics institutes there are groups whose activities and research are devoted to specific medical applications as well as to patient treatment, for example at GSI (Germany), PSI (Switzerland), GANIL (France), HMI (Germany) or LARN (Belgium).Particle therapy involves aiming ionised particles at the targeted tumour. The ionization indiscriminately damages cell DNA. However, cancer cells are less able to repair themselves and are more affected by this damage.
The particles used include protons, neutrons or positively charged ions. Each type of particle has a different energy and can therefore penetrate the human body by different amounts. This is why different types of particles are used for different procedures. The most common type of particle therapy is proton therapy.
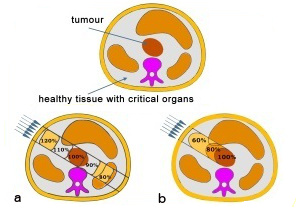
A fundamental problem of radiation therapy is the need to maximize the dose delivered within to the tumour while minimising harm to the healthy tissue around it. In electromagnetic radiations (X or γ rays), a large fraction of the dose affects the healthy tissue along the fascicle in front of and behind the tumour.
An improvement in radiation therapy is now achieved using high energy beams of particles (p, heavy ions) because for ion beams the doses increase with the penetration depth up to a maximum at the end of the particle range. Ion beam therapy allows a larger and more effective dose to be deposited in the tumour than any other type of external therapy.The image above right shows a comparison of two procedures. Photon therapy (a) deposits a high dose of radiation in the healthy tissue in front of the tumour. In the case of a particle beam (b), most of the dose is confined to the tumour.
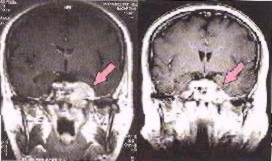
Image left shows a brain cancer scan before, and six weeks after radiotherapy with photons and Carbon ions.
To date, more than 50 000 patients worldwide have been treated with proton beams. The treatment of eye tumours by proton beams yields by far the best clinical result. Proton therapy is also ideal when the tumour is close to a critical organ as it can be aimed very accurately. The better conformity of the irradiated volume with the target volume, the better the results. This aslo holds true for heavy ions beams, where a superior conformity compared to protons can be achieved. Heavy ion therapy was pioneered in 1974 at Lawrence Berkeley Laboratory. The first treatments made use of Ar (argon) ions and then later, Si (silicon) and Ne (neon) ions. The irradiated tumours were close to critical organs in the brain, head or neck. The results were excellent and motivated the construction of dedicated Heavy Ion Medical Accelerators.
Brachytherapy is a form of radiation therapy where radioactive material is placed inside the body, close to the tumour. The advantages of this procedure are that the radiation does not have to travel from the outside of the body through healthy tissue to reach the tumour and instead only affects a localised area. This means that relatively high doses can be given with minimal risk. Also, the patient is mobile during the length of the treatment. The overall treatment is usually completed in less time than other procedures and so there’s less time for cancer cells to multiply in between treatment sessions.
Brachytherapy is a standard technique for some gynaecologic cancers such as cervical or prostate cancer and certain stages of head and neck carcinoma. For prostate diseases, various approaches have been used and these are mainly dictated by the isotope selected. 125I (with a half life of 60 days) and 103Pd (with half life of 17 days) are used for permanent implants. These isotopes can be produced by neutron capture in reactors. 103Pd can be produced more efficiently in cyclotrons (with proton beams of 14 MeV). More than 10 years of clinical data from the use of 103Pd in prostate brachytherapy exists in the USA. This clinical success, together with a lack of side effects, has made it a very popular choice for therapy.
The Sun emits visible light, infrared radiation that we feel as heat, and ultraviolet radiation that, unfortunately, can be dangerous. The ultraviolet radiation can cause skin melanoma (skin cancer). Skin melanoma is one of the most common causes of cancer and in 2008 for example has killed about 46,000 people worldwide.
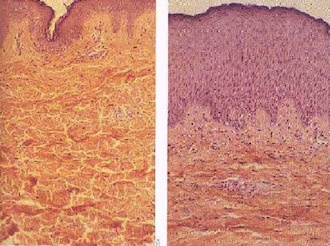
The rate of malignant melanoma diagnoses has quadrupled in the last 30 years. It is most commonly found in people with a family history of skin cancer, fair-haired and fair-skinned people and those older than 40. However, anyone can develop cancer regardless of race, age or genetics. Most skin damage occurs before the age of 20 but often doesn’t show up until the age of 40 so even if you can’t see yourself burning, you’re still damaging your skin. This is why it’s so important to wear sun cream and stay out of the Sun when it’s strongest (between 11am and 3pm).

